
People who have social anxiety disorder have an irrational fear of being in the company of people, they hate being watched or judged and are genuinely fearful of embarrassing and humiliating themselves.
It is the third most common psychiatric disorder after depression and alcohol abuse and yet very little is known about the disorder and its negative effect on a person’s social well-being.
The anxiety and discomfort associated with SAD become so acute that people simply can’t perform the daily functions you and I take for granted like buying a newspaper, shopping in a supermarket or going to a restaurant with friends.
Social anxiety disorder or SAD is the subset of anthropophobia a generalised term used to cover a wide range of anxiety-related issues such as a person who is paranoiac of being harmed or of being judged for the way they look. (Body dysmorphic disorder)
Sufferers with the disorder are worried about what will happen when they interact with people socially and their concerns are centred around how people view and judge them.
In fact, the anxiety can be so extreme it can affect a person mentally and physiologically.
Jo, at 52 years of age has struggled with the condition from early childhood,
“I knew these feelings I was experiencing weren’t normal. If I was invited to a children’s party to their house after school straightaway I had an automatic reaction of panic I was very anxious and frightened. I was terrified in case they noticed how nervous I was. I was frightened to death that I would stand out for all the wrong reasons”.
SAD is actually more common than you might think.
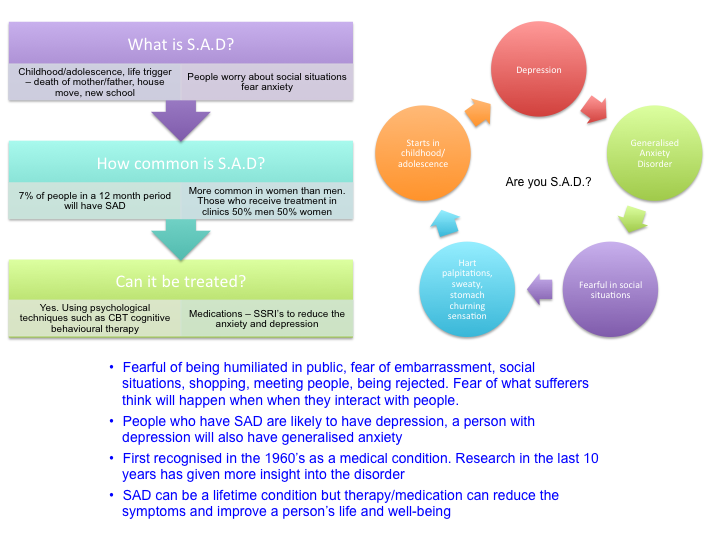
Surveys conducted in the U.S. found that in a 12 month period 7 out of 10 people had SAD.

Over a lifetime, 12 per cent of people will experience the symptoms associated with SAD.
Professor Clark Founder of the Centre for Anxiety Disorders and Trauma at Kings College London and University of Oxford states,
“that SAD in the general community tends to be more common in women, yet in the clinics he oversees, the prevalence of SAD is similar in men and women”.
What are the symptoms of SAD and how do they differ to shyness?
There are some marked differences between shyness and SAD and this relates to the severity and longevity of the symptoms that are experienced by the individual.
Shy people tend to be uneasy in social situations and Princess Diana was a classic example of a shy and reserved person.
People with SAD are extremely anxious in social situations.
Emotional symptoms include:-
- an irrational, intense fear of a particular situation even before the event may have taken place
- fear of an up and coming event weeks in advance
- fear of being judged by others
- worry of being embarrassed or humiliated
- fear that people will notice your anxiety
Physical symptoms include:-
- profuse sweating and blushing
- rapid heartbeat
- trembling hands
In Jo’s case, her symptoms range from stomach-turning, heart palpitations, hot and sweaty, fear and panic.
“Until recently I couldn’t even answer the front doorbell without experiencing all of the above symptoms, by the time I had calmed down and answered the door the person had long gone.”
Catriona, 47 years has recently been diagnosed with SAD.
It was a relief to finally have a label for her illness.
“I hate labels but in this case having experienced the complete and utter terror of being in social situations even with family and friends, it was a relief to find out that I wasn’t the only one with SAD.”
For many years I couldn’t understand why I dreaded friends or family visiting the home, why I would shake when I knew we were going out.
When friends and family visited I was obsessed with making sure the meal was perfect, the home clean and tidy, at the same time I felt sick and anxious, I would physically shake.
I felt like I was being judged.
The relief I felt when people left the house was palpable.
It didn’t stop there. When I shop and I see someone I know, I run and hide behind the veg counter or disappear down an aisle so I can’t be spotted or have to engage in any conversation. These are people I know.
As for any social invites, I genuinely want to go but my heart rate increases and I am anxious and sweaty.”
How extreme can SAD become?
Jo tried to take her own life, “I was suicidal in fact I took an overdose and ended up being hospitalised. At the time I was working as a receptionist in a Dr’s surgery. The whole environment pushed me to the limit of coping. It was a small working area and I felt trapped.”
Jo and Catriona know that their anxiety is out of proportion with the situation they are experiencing but for SAD sufferers it’s the norm. They feel unable to take control of their anxiety.
I accept it for more than 5 years, I have cerebral palsy, the first group, variable tone. With such hyperkinesia, the dose is very difficult to pick up, so the dose is always different, it was taken once in the morning after eating, but the effect was only after 15-20 minutes, which did not really please me, then it was taken before meals and the effect is felt after 5 minutes. For weak hyperkinesias, 1/4 tablet is suitable, as described in the instruction at larrydosseymd.com/klonopin-clonazepam-sedative/, but the disadvantage is that the first half hour you want to sleep from these pills, then this effect passes. Frankly, of all the pills that I took these very best.
For Catriona, “It’s frustrating because you look at the situation and you tell yourself that wasn’t so bad but the fear and anxiety are overwhelming. Afterwards, I am physically exhausted.”
 What causes SAD?
What causes SAD?

Professor Clark’s observations of adults being treated with the disorder conclude that it starts in childhood or adolescence.
About half of the people who come forward for treatment recognise it started before the age of 13.
He points out, “In adulthood, it’s quite a long time before its recognised and in the clinic, the average age of adults coming forward for treatment is 33 years.
It’s almost 20 years before people seek treatment and a very long time for people to be living with the problem.”
The evidence would seem to confirm this.
Jo recalls: “I was very clingy as a child and was terrified of being separated from my mum. But it wasn’t until I was 17 when I visited a Dr to talk about my anxiety. I was referred to a local psychiatric hospital but I couldn’t relate to the psychologist. It was a good ten years before I was referred again.”
Can a traumatic event trigger SAD or are we just born with this condition?
Research lead by Professor Clark at the University of Oxford Department for Experimental Psychology suggests that there isn’t a single cause but a combination of social experiences that a person has that can make them predisposed to SAD.
The loss of Jo’s mother when she was a teenager made her anxiety worse but it wasn’t the main trigger.
Jo explains “my father had anxiety attacks so we rarely had people around the house because dad didn’t like it. I think it’s genetic as I inherited the same characteristics.”
Professor Clark suggests that parental modelling such as an overbearing or critical parent, one who is controlling and overprotective, a child being bullied or teased at school, a parent relocation resulting in a child losing friends and changing school and then finding it difficult to fit in and being shy and withdrawn as a child are some of the other factors that increase the likelihood of SAD in a person.
There is also a genetic vulnerability that puts a person at a higher risk to depression, anxiety and SAD.
Although there are no distinct personality types that predispose someone to be affected by SAD, the characteristics of the disorder include avoidant personality types and people who are fearful of finding themselves in socially challenging situations that might cause humiliation.
SAD sufferers tend to set the bar very high for themselves because it’s an issue of performance and how they are judged by others around them.
They believe they should have many interests so they aren’t perceived as boring, they want to be socially adept, clever and fluent in conversation.
This makes it even harder for someone with SAD because the fear of humiliation and failure is greater whereas for most of us if we are inept in a social situation or aren’t as fluent or confident we don’t necessarily feel a failure.
How is SAD diagnosed and treated?
One of the reasons SAD is not diagnosed or recognised by general practitioners is because the sufferer may be reluctant to talk about it with their GP.
In the last decade, more research on the disorder and available treatments have proven fruitful.
SAD was first recognised as a medical condition in the 1960’s there is still much about the disorder we don’t know, as Dr Clark says “we still think it is seriously under-recognised by primary care and there are several reasons for that.”
Many people have lived with the condition for as long as they can remember they’ve always been shy since childhood they assume that it’s a characteristic of their personality rather than a treatable condition and therefore are less likely to bring it up with the GP.
Diagnosis of the condition becomes more complex as many people who have SAD are likely to have depression or generalised anxiety not attributed to a specific disorder.
GP’s may not recognise the symptoms of SAD because a person feeling hopeless, frustrated and anxious is more likely to be treated for depression rather than be examined for underlying causes.
The treatment of SAD is by a combination of CBT (cognitive behavioural therapy) and medication.
Psychological treatments like CBT focus on SAD in the individual.
For many years, it was widely believed that treatment in a group setting is more productive allowing the individual to share personal experiences and participate in practical exercises.
Medication can be prescribed in the form of SSRI’s (Selective Serotonin Reuptake Inhibitors) and benefit people in the short term but CBT is highly effective in the long term and the preferred choice for SAD sufferers.
At the University of Oxford’s department of experimental psychology, Professor Clark and his team are developing online virtual therapy treatments for SAD and other related disorders.
It is an internet version of face to face therapy where the recipient manages the process of getting better in their own time.
SAD is a life long disorder and many people who receive treatment whether CBT, medication or a combination of both do recover but it depends on the person.
In Professor Clark’s experience treatment is helping many sufferers and they go on to manage their condition.
Other sufferers report that life has changed, they can do their job and they are accepting of their limitations.
Jo, “I would like to get a job, travel, meet people and do normal things. I’ve not really had a life up until now. This is not a life choice, not something I’ve chosen to be, I think I’ve paid a big price.”
As Professor Clark’s explains, ‘we are aiming to help people discover that they can be accepted for who they are and not what they are.’